Online Health History Form
Patient
Experience
Our Orthodontists Are Dedicated to
Providing the Best Patient Experience.
Our top priority is to provide you with the highest quality of orthodontic care in a warm and friendly environment.

#csorthodontics
Don't Wait

Actual Patient
Request a Complimentary Exam Today!
Our office provides high level orthodontic services by offering comprehensive solutions for all treatment types.
What our patients are

Best place ever! I never have pain in my mouth after every visit and my treatment is looking very good. Stuff in this clinic is absolutely incredible, everybody is very kind and great services!!

Andres A.
My son and I were at his location yesterday. Dr. Carroll and his entire staff are extremely professional. The service and care from beginning to the end of the appointment was very informative as to what treatment my son will need in the near future. We highly recommend Dr. Carroll.
JR B.
By far the best!! Dr. Carroll and his staff are amazing. They are friendly and kind. They take their time to make my son feel comfortable and explain everything I need to know. My son loves going here. Also, they are not out to do a bunch of stuff you don't need. I initially went here for a second opinion and I am so happy I did. It saved me a lot of money and was less traumatic for my son. I can't thank them enough!
Mike W.
By far the best!! Dr. Carroll and his staff are amazing. They are friendly and kind. They take their time to make my son feel comfortable and explain everything I need to know. My son loves going here. Also, they are not out to do a bunch of stuff you don't need. I initially went here for a second opinion and I am so happy I did. It saved me a lot of money and was less traumatic for my son. I can't thank them enough!
Lora A.
Dr. Aaron Carroll and his team are wonderful! 6 out of 5 stars if I could. He helped multiple members of our family and results were fantastic. Clean office and very professional care. Highly recommend!
Mina A.
I love this office soon much. JESS IS LITERALLY THE BEST. How often do people look forward to getting their braces tighten? Meee bc I love Dr Carroll and all of his people. I feel right at home with them!
Wara R.

Actual Patient
Follow Us
Instagram 








It’s our sweet Nadia’s birthday! 💗🎉 We had so much fun celebrating her today and are so thankful for her! Wish her a happy birthday below!
#HappyBirthday #OfficeBirthday #LoveWhereYouWork #Orthodontist
1 week ago

✏️ First day of school? Ready ✅
🎒 New supplies? Ready ✅
😁 New smile? READY! ✅
This transformation is the perfect way to start a brand-new school year. ✨
#BackToSchoolSmile #SmileTransformation #CarrollandSuttonOrthodontics #Braces #BeforeandAfter
1 week ago






⚽️🏆 Orthodontic World Cup Red Cards & Yellow Cards 🏆⚽️
Here are some fouls and warnings! 🚩
Here’s the call from the orthodontic referee 🦷👇
🔴 Stopped wearing your retainers
➡️ Retainers keep your teeth in place; wear them as directed to protect your winning smile! Otherwise your teeth will shift!
🟡 Forgot your elastics for one night
➡️ It happens sometimes! Just make sure to get back on track and keep wearing them consistently.
🔴 Missing appointments
➡️ Regular visits keep your treatment moving in the right direction! Missed appointments put you behind.
🟡 Forgot to floss
➡️ It happens! Just get back into the habit to keep your teeth healthy and braces looking great!
🔴 Eating foods you shouldn’t with braces
➡️ Eating foods you should be avoiding can break brackets and slow down treatment.
🔴 Not wearing aligners for 22 hours a day
➡️ This will delay your treatment. Make sure to always wear them exactly as instructed!
⚽️ Keep your smile goals on track and avoid those red and yellow cards! 🦷🏆
#CarrollAndSuttonOrthodontics #WorldCup #BracesTips #SmileGoals
2 weeks ago



🎉 Welcome to our Smile Hall of Fame! 🎉
These amazing patients have officially completed their smile journeys, and we couldn't be more excited to celebrate them! 😁✨ Congratulations on all of your hard work, dedication, and beautiful new smiles! We're so proud of each and every one of you! 🦷💙
Thinking about starting your own smile journey? We'd love to meet you! Schedule your FREE consultation today and let's create a smile you'll love.
📞941-257-2000
#SmileHallOfFame #BracesOff #Orthodontics #CarrollAndSuttonOrthodontics #SmileJourney #NewSmile #Braces #SmileGoals #CelebrateYourSmile
2 weeks ago

🍎✏️ Nominations are still open! ♥️
This July, we’re celebrating the amazing educators in our community by giving FIVE deserving teachers each a $100 Amazon Giftcard to help them get ready for the upcoming school year 📚✨
🍏 To nominate a teacher, simply comment their name, school, and grade they teach below 👇
Nominations are open all month long, and our 5 winners will be selected at the beginning of August! 🩵
#TeacherAppreciation #WeLoveOurTeachers #Community #Orthodontist #Orthodontics #SouthwestFlorida
3 weeks ago

Happy Workiversary, Carley! 🌸✨Your positive energy is magnetic & you make the office brighter each day! ☀️ We’re so thankful you’re a part of our CSO 🦈 fam! 🩵🤍🦷
3 weeks ago
We understand it happens sometimes! Make sure to always let us know when you break a bracket so you can come in and get it fixed!
#funatwork #carrollandsuttonorthodontics #funny #lovewhereyouwork
3 weeks ago
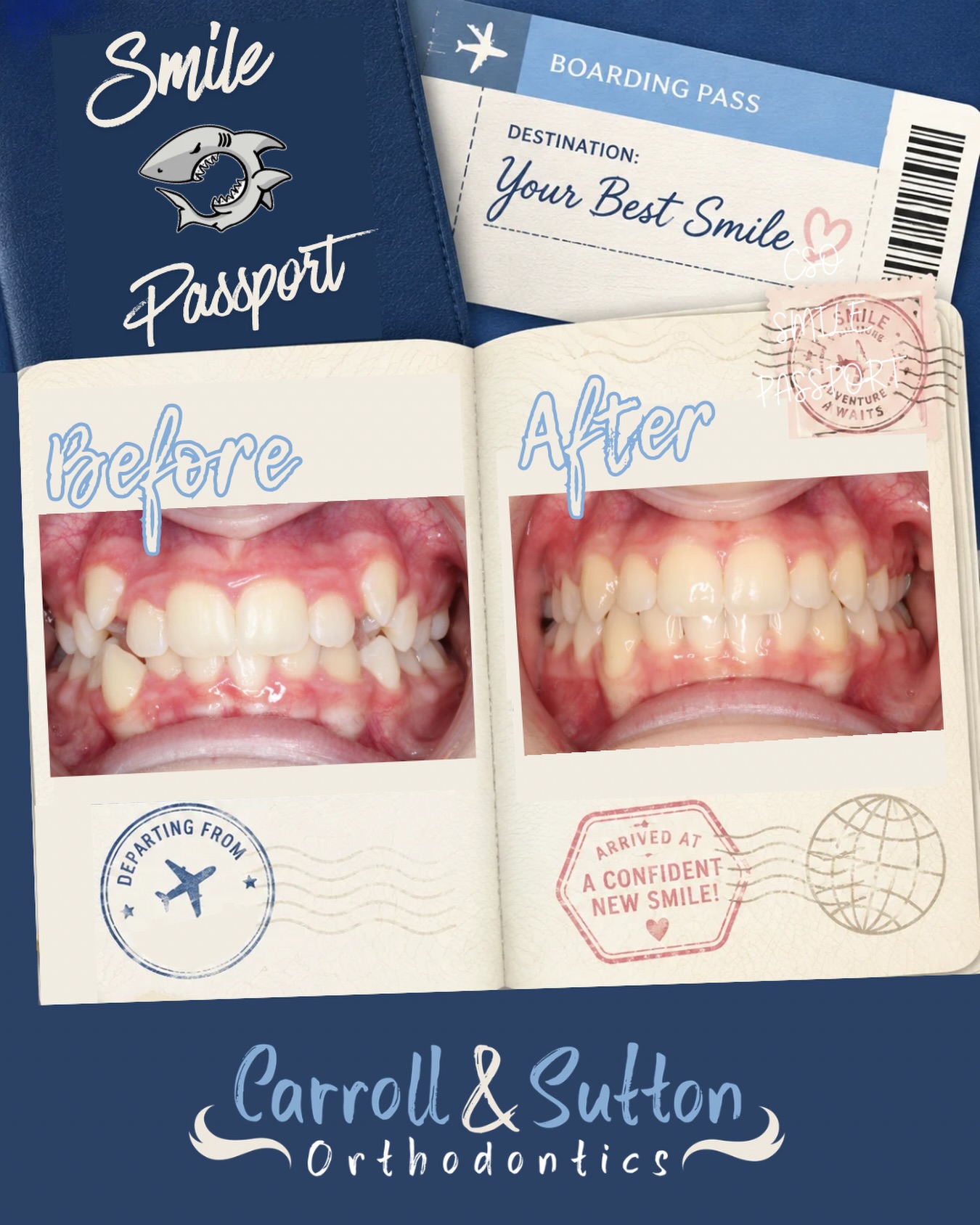
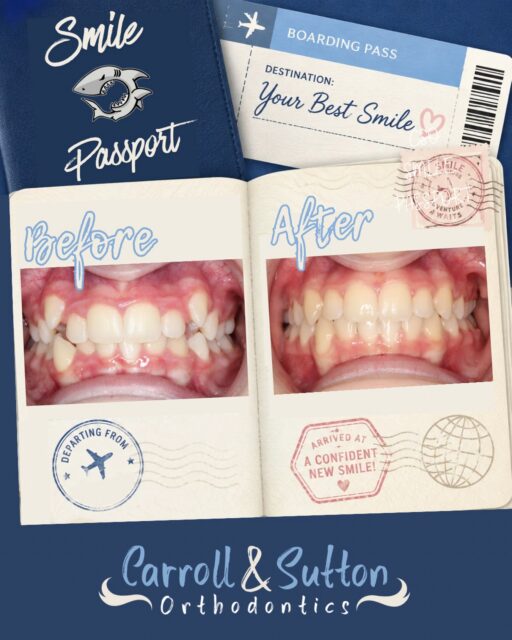
✈️ Next Stop: New Smile! 😁
This is a smile journey worth stamping! 🌎✨ From the first appointment to the final reveal, this smile has officially arrived at its final destination! 🧳🦷
🤙🏼 Book your complimentary consultation today to start your smile adventure!
#Orthodontics #SmileReveal #BeforeandAfter #SmileTransformation #SouthwestFloridaOrthodontist
3 weeks ago
facebook 
Tiktok 
Don't Wait
Request a Complimentary Exam Today!
Our office provides high level orthodontic services by offering comprehensive solutions for all treatment types.
What our patients are
Best place ever! I never have pain in my mouth after every visit and my treatment is looking very good. Stuff in this clinic is absolutely incredible, everybody is very kind and great services!!
Andres A.
My son and I were at his location yesterday. Dr. Carroll and his entire staff are extremely professional. The service and care from beginning to the end of the appointment was very informative as to what treatment my son will need in the near future. We highly recommend Dr. Carroll.
JR B.
By far the best!! Dr. Carroll and his staff are amazing. They are friendly and kind. They take their time to make my son feel comfortable and explain everything I need to know. My son loves going here. Also, they are not out to do a bunch of stuff you don't need. I initially went here for a second opinion and I am so happy I did. It saved me a lot of money and was less traumatic for my son. I can't thank them enough!
Mike W.
By far the best!! Dr. Carroll and his staff are amazing. They are friendly and kind. They take their time to make my son feel comfortable and explain everything I need to know. My son loves going here. Also, they are not out to do a bunch of stuff you don't need. I initially went here for a second opinion and I am so happy I did. It saved me a lot of money and was less traumatic for my son. I can't thank them enough!
Lora A.
Dr. Aaron Carroll and his team are wonderful! 6 out of 5 stars if I could. He helped multiple members of our family and results were fantastic. Clean office and very professional care. Highly recommend!
Mina A.
I love this office soon much. JESS IS LITERALLY THE BEST. How often do people look forward to getting their braces tighten? Meee bc I love Dr Carroll and all of his people. I feel right at home with them!
Wara R.
Actual Patient
Follow Us
Instagram
It’s our sweet Nadia’s birthday! 💗🎉 We had so much fun celebrating her today and are so thankful for her! Wish her a happy birthday below!
#HappyBirthday #OfficeBirthday #LoveWhereYouWork #Orthodontist
1 week ago
✏️ First day of school? Ready ✅
🎒 New supplies? Ready ✅
😁 New smile? READY! ✅
This transformation is the perfect way to start a brand-new school year. ✨
#BackToSchoolSmile #SmileTransformation #CarrollandSuttonOrthodontics #Braces #BeforeandAfter
1 week ago
⚽️🏆 Orthodontic World Cup Red Cards & Yellow Cards 🏆⚽️
Here are some fouls and warnings! 🚩
Here’s the call from the orthodontic referee 🦷👇
🔴 Stopped wearing your retainers
➡️ Retainers keep your teeth in place; wear them as directed to protect your winning smile! Otherwise your teeth will shift!
🟡 Forgot your elastics for one night
➡️ It happens sometimes! Just make sure to get back on track and keep wearing them consistently.
🔴 Missing appointments
➡️ Regular visits keep your treatment moving in the right direction! Missed appointments put you behind.
🟡 Forgot to floss
➡️ It happens! Just get back into the habit to keep your teeth healthy and braces looking great!
🔴 Eating foods you shouldn’t with braces
➡️ Eating foods you should be avoiding can break brackets and slow down treatment.
🔴 Not wearing aligners for 22 hours a day
➡️ This will delay your treatment. Make sure to always wear them exactly as instructed!
⚽️ Keep your smile goals on track and avoid those red and yellow cards! 🦷🏆
#CarrollAndSuttonOrthodontics #WorldCup #BracesTips #SmileGoals
2 weeks ago
🎉 Welcome to our Smile Hall of Fame! 🎉
These amazing patients have officially completed their smile journeys, and we couldn't be more excited to celebrate them! 😁✨ Congratulations on all of your hard work, dedication, and beautiful new smiles! We're so proud of each and every one of you! 🦷💙
Thinking about starting your own smile journey? We'd love to meet you! Schedule your FREE consultation today and let's create a smile you'll love.
📞941-257-2000
#SmileHallOfFame #BracesOff #Orthodontics #CarrollAndSuttonOrthodontics #SmileJourney #NewSmile #Braces #SmileGoals #CelebrateYourSmile
2 weeks ago
🍎✏️ Nominations are still open! ♥️
This July, we’re celebrating the amazing educators in our community by giving FIVE deserving teachers each a $100 Amazon Giftcard to help them get ready for the upcoming school year 📚✨
🍏 To nominate a teacher, simply comment their name, school, and grade they teach below 👇
Nominations are open all month long, and our 5 winners will be selected at the beginning of August! 🩵
#TeacherAppreciation #WeLoveOurTeachers #Community #Orthodontist #Orthodontics #SouthwestFlorida
3 weeks ago
Happy Workiversary, Carley! 🌸✨Your positive energy is magnetic & you make the office brighter each day! ☀️ We’re so thankful you’re a part of our CSO 🦈 fam! 🩵🤍🦷
3 weeks ago
We understand it happens sometimes! Make sure to always let us know when you break a bracket so you can come in and get it fixed!
#funatwork #carrollandsuttonorthodontics #funny #lovewhereyouwork
3 weeks ago
✈️ Next Stop: New Smile! 😁
This is a smile journey worth stamping! 🌎✨ From the first appointment to the final reveal, this smile has officially arrived at its final destination! 🧳🦷
🤙🏼 Book your complimentary consultation today to start your smile adventure!
#Orthodontics #SmileReveal #BeforeandAfter #SmileTransformation #SouthwestFloridaOrthodontist
3 weeks ago